Flixborough
revisited
NOTE: This webpage was first posted in January
2005 and, slightly abridged, appears in The Chemical Engineer
(April 2005). It has been modified for consistency with the
published version - save for Figure Nos. 7-10 that continue the
Figs 1-6 sequence of Flixborough
– Some Additional Lessons ("SAL")
and that two additional illustrations in the published version
appear in Flixborough
– FAQs.
In
June 1974, a 2-year-old caprolactam plant near Flixborough was
destroyed by a major explosion. Its shock waves echoed all around
Britain as neighbours of similar or older plants deluged
politicians with fears about nearby installations. Within days,
the government decided that a Public Inquiry was necessary to
allay public concern.
Fig. 7 Photograph of Section 25A at a late stage in its
construction
Its
outcome seemed a foregone conclusion. It was obvious that a
temporary by-pass line had jack-knifed and ripped away its
bellows connections to the 28" nozzles at both ends - and
never any doubt that the explosion was fuelled by a major escape
of superheated cyclohexane through these two open nozzles.
Officially
the Public Inquiry was asked to “establish the causes and
circumstances of the disaster.” However, as the
circumstances seemed unique, it was anticipated that the Court of
Inquiry would reassure the public that there was nothing to fear
from all other chemical plants. At that time (June 1974), there
was near-universal agreement that the 20" line was the sole
cause of the disaster (the so-called 20" line hypothesis).
Fig. 8 Court Plate 8 and a photograph of the 20" line
after explosion
To
demonstrate their hypothesis, the Court commissioned a replica 20"
line to be fabricated and connected by replica bellows between
two of the remaining reactors, to simulate what was thought to
have happened. It was announced, in advance of the opening of the
Public Inquiry, that the film of this simulation would be made
available publicly and would demonstrate what had caused the
explosion.
There
was, however, a dissenting voice. Dr. Keith Gugan, an experienced
accident investigator from Burgoynes, had found an 8" line
that, from its petal shaped fracture, he deduced had burst
through creep failure under pressure. He argued that this would
have occurred before the 20" line had jack-knifed (and
relieved the system pressure) and that that this pre-event must
have been the initiating cause of the disaster. In the jargon of
the Court, his event sequence became known as the 8" line
hypothesis.
When
the Court convened and heard eye-witness evidence from the
laboratory, it quickly became apparent that no-one had seen the
20" line fail (although it was visible from the laboratory)
and that all witnessed something other than the massive escape of
gas before the main explosion. Their accounts suggested that
there must have been one or more pre-events that activated the
fire siren at least 10 seconds before the jack-knife failure of
the 20" line and at least 30 seconds before the main
explosion.
Then,
a few days into the hearings, the Court conducted their
simulation test. As predicted, the 20" line did fail when
extra internal pressure was applied – but not in the way
expected. Instead of tearing away from the 28" nozzles, the
line merely distorted (‘squirmed’) with both bellows
connections left intact (Fig. 3a in "SAL"). Their
simulation, specifically designed to show that an over-pressurised
20" line initiated the train of events, actually showed that
an external force, applied from above, was needed to cause the
jack-knife. Scientific objectivity then went on hold as the Court
desperately tried to rescue its preferred hypothesis.
This
was not their only concern. By then it was known that something
unusual had happened in an overhead bank of fin-fan coolers.
Whilst most were crushed in situ when the plant structure
was felled by the main explosion, two rotors had flown upwards
and at right-angles to the main blast (Fig. 5A in "SAL"),
landed outside the structure (Fig. 7) and then were covered with
soot from the flash fire (that occurred concurrent with the main
explosion).
Fan
Rotor 8 (landed past roadway)
Fan Rotor 9 (landed on roadway)
Fig. 9 Fan rotors 8 and 9 after explosion, covered in soot
from flash fire
So,
two weeks into the public hearings, the Court’s single event
hypothesis faced a major challenge. It had to explain more than a
dozen eye-witness accounts of at least two events before the main
explosion – and, even more difficult, how creep failure in
the 8" line and an explosion in the fin-fan coolers could
have followed afterwards.
In
retrospect it is obvious that the proceedings should have been
adjourned to allow time for scientific tests to resolve the
technical issues. Unfortunately, the Court had already ‘gone
public’ in favour of its 20" line hypothesis. The Court
decided to hear evidence on various peripheral issues whilst it
conducted new investigations that, they hoped, would restore
scientific credibility to their preferred hypothesis.
Simultaneously,
various other issues of concern were under study – most of
which have been recorded in research reports and/or presented at
the IChemE symposium held at the end of 1975. The most relevant
of these for the causation issue concerned “zinc
embrittlement of stainless steel” – and were
conducted by Mr. Orbons of DSM.
His
findings explained why fin-fan coolers that were made from
stainless steel had shattered (whilst those from mild steel
remained intact) and revealed, inter alia, that the
explosion in the stainless steel fin-fan coolers (numbers 7-10)
could have been caused by a fire of only a few seconds. The Court
accepted that this caused the fin-fans’ explosion - but not
that it must have occurred before the main explosion.
Meanwhile,
the 8" line had remained in the care of the Court but (as
they did not think it relevant to causation) not available for
metallurgical examination. Eventually, just before the Christmas
recess, when the Court was satisfied it had the evidence it
needed to complete its findings, it was released for forensic
tests by Sir Alan Cottrell and Professor Peter Swann.
Their
creep rupture tests were conclusive. These showed that the
metallographic and morphological characteristics of the failure
of the 8" line at its elbow were consistent with failure
after about 4 minutes between 950°C and 1000°C at its normal
working pressure (equivalent to 7.4kg/mm2). This is
illustrated in Figure 10 (copied from The Chemical Engineer,
April 1976, page 270).
Fig. 10 Examples of w-type creep cavities in steel of 8”
line
Given
that tens of tonnes of cyclohexane would have escaped from the 28"
nozzles within 4 minutes of the 20" line jack knife (more
again from equipment damaged by the main explosion within a
minute of the first event), it is inconceivable the normal
working pressure would have been retained in the 8" line for
4 minutes if, as argued by the Court, the 20" line was first
to fail. Moreover, the direction of the applied stress was
consistent creep failure in an undistorted 8" line.
This was convincing evidence that the 8" line actually
failed before the 20" line.
Nor
was this all: Cottrell and Swann also determined the temperature
profile of nearby sections of the 8" line (Fig. 6A), showing
a rapid fall from 950°C at the intrados of the elbow to less
than 750°C only a few feet away. This confirmed that something
other than the general fire after the explosion must have been
responsible for highly-localised heating at the intrados (hypothesised
in Fig. 6B).
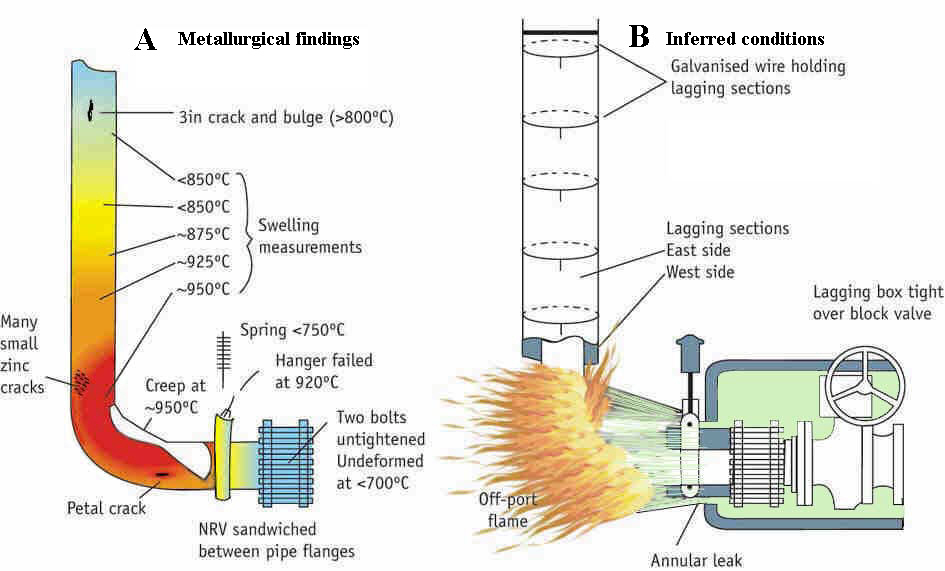
Figure 6 - reproduced from tce, May 1976
Lacking
further forensic evidence, the missing details of the hypothesis
then had to be completed by a sequence of credible conjectures:
ü
There was a gasket leak at the nearby non-return valve (a
credible scenario as two bolts were found to have been left
untightened).
ü
This leak resulted in an escape of cyclohexane that was directed
at the intrados of the elbow from an essentially intact lagging
box.
ü
The escape ignited and preferentially heated the sections of
lagging over the intrados and nearby.
ü
The lagging disintegrated and the zinc-coated wires (used to keep
the lagging in place) contacted (or came very close to) the
stainless steel pipe.
ü
The 3" crack (top of Fig. 6A) was created instantly by zinc
embrittlement.
ü
With cyclohexane now escaping on either side, the intrados of the
elbow became vapour-locked and its temperature rose to 950°C.
ü
After another 4 minutes, creep failure occurred at the petal
crack.
Having
conjectured this scientifically credible sequence of events that
conformed to the unimpeachable hard forensic evidence, the eye-witness
statements were reviewed (Figures 4 and 5A of "SAL").
Using the main explosion as the fixed time origin and working
back by re-enactments of what each witness remembered seeing,
hearing and doing just beforehand, it was easy to establish that:
ü
More than 20 eye-witnesses saw flames up to ¾ minute earlier.
ü
Of these, 8 described a vertical flame consistent with an
emission from the ruptured elbow of the 8" line up to 25
seconds earlier.
ü
One eye-witness (at location 15 of Fig. 4 ) reported seeing, at
least 25 seconds earlier, an object consistent with the
trajectory, shape and size of Fan Rotor 9 in flight.
ü
The 7 laboratory eye-witnesses (Fig. 5A) were alerted at least 32
seconds earlier and were running for safety within 10 seconds (without
having seen the 20" line collapse).
In
all, over forty eye-witnesses provided statements for scrutiny.
None contradicted the 8" line hypothesis: several
provided strong confirmatory evidence and helped to determine the
timing of events. From the standpoint of science, the debate
ended with the forensic metallurgical findings. If the sole
consideration for the Public Inquiry was to find the truth, it
would have endorsed this multi-event and multi-cause explanation.
But
there was a problem. The 20" line hypothesis did not
blame anyone outside Nypro and was preferred by the process
licensors and plant constructors, the Factory Inspectorate and
everyone already on public record in its favour. These were
pressing commercial, institutional and personal objections to the
8" line hypothesis. None of the parties represented
at the hearings would benefit if it were adopted.
Its
adoption would have obliged the Court to highlight a frightening
large number of defects in plant design and construction (loose
bolts, gasket integrity, vulnerability of stainless steel in
contact with zinc, the hugely damaging potential of a jet fire,
an excessive inventory of superheated cyclohexane). These would
have been unpalatable findings for a public looking to the Court
for reassurance.
So
the Court held firm. Their report reasserts (Para. 209) that the
20" line was the sole item at fault: “The disaster
was caused by the introduction into a well-designed and
constructed plant of a modification which destroyed its integrity”.
With the hindsight of maturity – though I did not think so
at the time – I concede that they may have had some excuse
for their technically implausible conclusion.
If
they had endorsed the more credible hypothesis, with all its
attendant lessons, it could have exacerbated fears about the
location of chemical plants. The Nypro plant was ½ mile from the
nearest village (Flixborough) yet 72 out of its 79 houses were
damaged. It was thought to be one of the most modern plants in Britain
at that time and built in accordance with the best practice of
the day. If two loose bolts initiated the Flixborough events, was
anyone safe living close to a chemical plant?
These,
I am sure, are the reasons why the Court reached its
scientifically perverse decision. They were impelled to blame the
totally unsuitable 20" line as a one-off cause of the
disaster - and give the rest of the Nypro plant (and, by
implication, all others in Britain) a clean bill of health. This
decision was predictable and signalled well in advance of their
Report.
Their
predicament had been explained to me, weeks before the hearings
ended, by the Secretary to the Inquiry, a senior Factory
Inspector of high personal integrity who had been present
throughout the proceedings. He advised me then to concentrate on
the lessons of the investigations and gave a pledge that the
Factory Inspectorate (then in transition to becoming the HSE)
would publicise all the lessons of Flixborough –
irrespective of the Court’s findings.
Bernard
O’Reilly kept his word and I took his advice. My main
efforts, after the official report was out, were to publicise the
lessons from the investigations. Within a few months the
Institution of Chemical Engineers had endorsed my personal
proposal that it sponsor a symposium on “The Technical
Lessons of Flixborough.”
It
was held on 16th December 1975 in Nottingham and its
papers published in the April/May 1976 issues of The Chemical
Engineer. My contribution, “Flixborough – Some Additional
Lessons”, reprinted for this website, created so much
interest that several hundred extra copies were reprinted as a tce
supplement. Although it focused on the lessons for the future and
was not meant as a backward-looking review of the causation
hypotheses, much of this interest stemmed from its implicit
explanation of (what tce termed) the “main
alternative theory to that put forward by the Court”.
Today,
thanks to the efforts of an indefatigable Ralph King and an
unwavering Jim Venart, it remains common knowledge that the Court
of Inquiry did not win universal approval. Thankfully, throughout
the past thirty years, safety professionals have ignored the
central conclusion of the Public Inquiry (Para. 209) and
concentrated on its ‘unofficial’ lessons. One example
will suffice: the concept of “Inherent Safety”.
This
supposed “well-designed” plant had 200 tonnes of
superheated cyclohexane circulating without a single ESD
isolation valve to reduce an escape. There was no way the plant
operators could contain a leak, irrespective of its cause or
location. Had the IChemE (and, notably, Trevor Kletz) accepted
the Court’s findings, the concept of “Inherent Safety”
– now an integral feature of design safety philosophy -
would not have seen the light of day.
For
further details, see the original “Flixborough – Some Additional
Lessons”.
John
Cox, January 2005